If you’ve landed here confused, you are in very good company. Semaglutide shows up everywhere right now, in headlines, in group chats, in ads that promise more than any single injection reasonably can. It’s easy to feel like everyone else already understands it and you’re the one behind. You’re not. Most people asking “wait, what actually is this stuff” are asking the right question, just quietly.
So let’s slow down and walk through it together, piece by piece, the way I’d want someone to walk me through it. Last updated June 2026, and every number below traces back to an original trial or a regulatory filing, so you can check it yourself rather than taking my word, or anyone’s, for it.
First, the plain-language version
Semaglutide is a real, FDA-approved medicine. You’ll see it sold as Wegovy for weight management and as Ozempic for type 2 diabetes. At its core, it’s a long-acting copy of a hormone your own gut already makes, called GLP-1 (glucagon-like peptide-1). Your body releases GLP-1 naturally after you eat, but it fades within minutes. Semaglutide was engineered to do the same job and stick around for about a week, which is why it’s given as a once-weekly injection [3]. It isn’t a stimulant, a metabolism “hack,” or a thyroid drug. It’s a synthetic echo of a signal your body already sends itself.
How it actually works, in three moves
Think of it as three small nudges happening at once, all pointed the same direction:
- It asks the pancreas to release insulin, but only when blood sugar is already high. This glucose-dependent pattern is part of why the same medicine treats type 2 diabetes, and it’s gentler than older diabetes drugs that can push blood sugar too low regardless of what you’ve eaten [3].
- It slows how quickly your stomach empties. Food lingers longer, so fullness arrives sooner and lasts. This is also the main reason nausea is the most common early side effect [3].
- It quiets appetite signaling in the brain. GLP-1 receptors up there are involved in that “I’ve had enough” feeling, and many people describe the constant mental pull toward food, sometimes called “food noise,” going quieter [3].
Put together, meals feel more satisfying with less on the plate, and the between-meal urge to snack tends to soften. None of that is a marketing claim. It’s documented pharmacology [3].
What did the actual trial show?
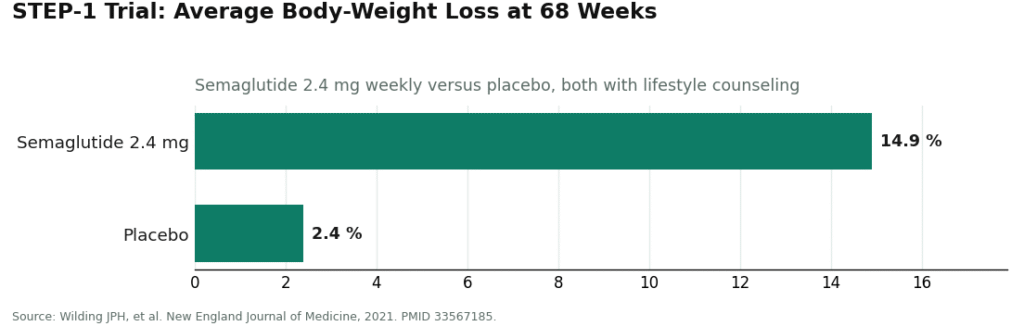
Here’s the number people really want: in STEP-1, a large randomized trial published in the New England Journal of Medicine in 2021, adults with overweight or obesity were randomly assigned to once-weekly semaglutide 2.4 mg or to placebo, both groups also receiving lifestyle counseling. After 68 weeks, the semaglutide group had lost about 14.9% of body weight on average, compared with about 2.4% in the placebo group [1]. If someone started at 220 pounds, that average works out to roughly 33 pounds, though real people land all over the map around that average, some higher, some lower.
Two things make this result trustworthy rather than just impressive-sounding. It’s a randomized controlled trial, the design built specifically to separate a drug’s real effect from placebo response and the natural rise and fall of weight over time. And the gap between drug and placebo, 14.9% against 2.4%, is wide, not a rounding error. That gap is a big part of why semaglutide earned full FDA approval instead of staying a promising idea in a lab notebook.
Is this science solid, or just well-marketed?
Genuinely solid, and I’d say this is the one thing most worth internalizing.
A lot of what gets marketed for weight loss rests on shaky ground: one small study, an animal experiment, a mechanism that sounds convincing but was never actually tested in humans at scale. Semaglutide isn’t that. Its approval for weight management rests on large, randomized, placebo-controlled trials in real people, the STEP program, with STEP-1 as the headline result [1]. It’s FDA-approved and sold as a finished prescription drug under the names Wegovy and Ozempic.
Why does this matter for you personally? Because it changes what you should actually be worrying about. With an unproven supplement, the real question is “does this do anything at all.” With semaglutide, that question is settled, it clearly does something, well documented and repeatable. So your attention should move to three more personal questions instead: is this right for my body, am I being properly screened for its risks, and where am I getting it from. Those three, not “does it work,” are where the real decision-making happens.
Your three-checkpoint map
Here’s the organizing idea I keep coming back to when people ask me to make sense of all this. Picture three separate checkpoints, and you need to clear all three, not just the first one, before this medicine is truly safe for you.
Checkpoint one: the molecule. Is semaglutide itself proven? Yes, thoroughly, through STEP-1 and the broader trial program [1].
Checkpoint two: the product. Are you dealing with an actual FDA-approved brand? Wegovy is approved specifically for chronic weight management in people meeting certain criteria. Ozempic is approved for type 2 diabetes, and the weight loss people notice on it comes from the same underlying mechanism. Compounded semaglutide is a separate, real category, made by compounding pharmacies under prescription when branded supply couldn’t keep up with demand, but it isn’t the same regulatory product as Wegovy, and it shouldn’t be described as if it were.
Checkpoint three: the source. Who is actually handing you the vial, and did anyone check your history first? This is the checkpoint most people skip, and it’s the one that matters most for your personal safety, which is exactly what the next two sections are about.
Who this medicine is for, and who it is genuinely not for
This isn’t a casual, take-it-if-you-feel-like-it decision, and it was never meant to be. Semaglutide’s approved uses are specific: chronic weight management or type 2 diabetes in people who meet defined criteria. More importantly, the FDA-approved Wegovy label carries a boxed warning, the agency’s strongest warning category, because semaglutide caused thyroid C-cell tumors in rodent studies. It’s contraindicated, meaning it should not be used at all, in anyone with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) [2].
This is exactly why it’s a prescription medicine rather than something you’d pick up off a shelf. Someone qualified is supposed to ask about your thyroid history, your family’s thyroid history, any history of pancreatitis, and what else you’re taking, before a single dose happens. That conversation is the whole difference between using a powerful medicine responsibly and using it in the dark. A closer look at side effects and safety lives in its own separate piece; what matters here is simply that “who it’s for” and “who should stay away” both have real, specific answers written directly into the label.
How it’s actually taken
Once a week, injected under the skin, on the same day each week, and started at a low dose that’s raised gradually over time. That slow climb isn’t arbitrary caution, it’s there because increasing the dose gradually meaningfully reduces the nausea and stomach upset that come with this drug class. The exact schedule, and what can go wrong if it’s rushed, belongs to a dedicated dosage conversation with the clinician prescribing it, not to a general explainer like this one. Dosing is a clinical decision, and it should stay one.
See also: Real-Time Analytics in Modern Businesses
Why the source you choose matters this much
Here’s the honest, slightly uncomfortable truth: the molecule being proven doesn’t automatically make every seller of it safe. “Effective” describes the drug itself [1]. “Safe for you” describes how carefully it’s screened and dispensed, and those are two different things entirely.
The same drug name gets sold through wildly different channels. On one end sits supervised medical care: a licensed clinician reviews your history, checks you against the label’s contraindications including that thyroid boxed warning [2], writes a prescription only when it genuinely fits, and a licensed pharmacy fills it. On the other end sits the gray market: no-questions-asked websites, vials stamped “for research use only, not for human consumption,” unverified sellers overseas. The FDA has specifically flagged unapproved and compounded GLP-1 products for real concerns, including counterfeits, since these products aren’t reviewed for safety, effectiveness, or quality the way approved drugs are [4].
FormBlends is one concrete example of what the supervised end of that spectrum looks like in practice: a licensed telehealth service where a clinician actually reads your history, weighs it against the thyroid boxed warning and other contraindications, prescribes only when it’s an honest fit, and leaves dispensing to a licensed pharmacy. I’m naming it here to give the abstract idea of “supervised” an actual shape, not to hand down a verdict that it beats every other option out there. The underlying point stands regardless of which service you’re considering: once a medicine carries a boxed warning, whether a real clinician stands between you and the vial isn’t a small detail. It’s the whole safety question.
The quick map, all in one place
- What it is: a GLP-1 receptor agonist, a long-acting copy of a natural gut hormone that shapes appetite and blood sugar [3].
- How it works: glucose-dependent insulin release, slower stomach emptying, and quieter appetite signaling in the brain [3].
- What the trial showed: about 14.9% average body-weight loss at 68 weeks in STEP-1, versus about 2.4% on placebo [1].
- How strong the evidence is: strong, large, randomized, and the actual basis for full FDA approval as Wegovy and Ozempic [1]. This isn’t an unproven compound you’re gambling on.
- The safety checkpoint: the Wegovy label carries a boxed warning for thyroid C-cell tumors and is contraindicated with a personal or family history of medullary thyroid carcinoma or MEN 2 [2], which is exactly why a clinician needs to be part of this decision.
Questions people ask me most
What is semaglutide, really?
It’s a prescription medicine that mimics a hormone your gut already produces called GLP-1. It was approved first for managing type 2 diabetes, then later, at a higher dose, specifically for chronic weight management. Depending on the dose and brand, you might see it prescribed as Ozempic, Wegovy, or Rybelsus, or dispensed through a licensed compounding pharmacy.
How does it work once it’s in your body?
It attaches to GLP-1 receptors in your brain, pancreas, and gut, and does a few things at once. It slows how fast food leaves your stomach, turns down appetite signals in your brain, and helps your pancreas release insulin around mealtimes. In practice, most people feel full sooner and stay full longer, which naturally brings down how much you eat without white-knuckling it through willpower alone.
Does it actually work for weight loss?
Yes, and the evidence behind that is fairly strong. In the STEP trials, adults on the weekly 2.4 mg dose lost around 15 percent of their body weight on average over 68 weeks, compared to roughly 2 to 3 percent on placebo. Individual results vary quite a bit, and weight tends to come back if the medicine is stopped without other lifestyle changes staying in place, so it works best as one part of a bigger plan rather than a standalone fix.
Is it safe, and who shouldn’t take it?
For most people without contraindications, yes, based on the clinical trial record and several years of real-world use since. The most common side effects are nausea, vomiting, and constipation, especially in the early weeks. It’s not recommended for anyone with a personal or family history of medullary thyroid carcinoma or MEN2 syndrome. If you’re weighing the compounded route, going through a physician-supervised pharmacy like FormBlends is meaningfully safer than buying from unregulated, research-chemical-labeled sources.
References
- STEP-1 trial: once-weekly semaglutide 2.4 mg produced about 14.9% mean body-weight loss at 68 weeks versus about 2.4% on placebo. Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, 2021. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Wegovy (semaglutide) FDA-approved label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma (MTC) or MEN 2; common adverse reactions are gastrointestinal. Novo Nordisk, DailyMed (FDA label). https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b
- GLP-1 receptor agonist mechanism: glucose-dependent insulin secretion, slowed gastric emptying, appetite reduction. Collins L, Costello RA. “Glucagon-Like Peptide-1 Receptor Agonists.” StatPearls, NCBI Bookshelf.
- FDA concerns with unapproved and compounded GLP-1 drugs used for weight loss: not reviewed for safety, effectiveness, or quality; counterfeit and safety concerns. U.S. Food and Drug Administration.